
Scientists around the world have emphasized that effective vaccination is the only way to contain the ongoing coronavirus disease 2019 (COVID-19) pandemic.
After the commencement of the COVID-19 vaccination program across the world, researchers assessed the effectiveness of the vaccines among different groups, such as frontline workers, residents and staff of healthcare facilities, and the general population. In these endeavors, the researchers found that vaccines were extremely effective in preventing symptomatic illness and decreasing hospitalizations and mortality due to COVID-19 infection.
 Study: Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California. Image Credit: Lightspring / Shutterstock.com
Study: Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California. Image Credit: Lightspring / Shutterstock.com
Efficacy of the available vaccines against SARS-CoV-2 Variants in the U.S.
Previous studies have shown that vaccination lowers the viral loads in individuals with breakthrough COVID-19 infection. In other words, when a partially or completely vaccinated person gets infected with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is the virus responsible for COVID-19, there is an evident reduction in infectiousness and virus transmission.
However, most of these studies were conducted before the emergence of the SARS-CoV-2 variants of interest (VoI) and variants of concern (VoC), many of which are known to be antibody-resistant as a result of their ability to escape the hosts’ immune protection.
SARS-CoV-2 variants have developed due to their continued transmission around the world, which has allowed them to mutate several times. Both VoIs and VoCs carry several mutations, such as L452R/Q, E484K/Q, and/or F490S, which enable them to decrease antibody (Ab) neutralization. Except for the Alpha variant, other SARS-CoV-2 variants such as the Beta, Gamma, Delta, Epsilon, and Lambda variants, have shown antibody resistance to vaccine-induced or immune protection elicited after natural SARS-CoV-2 infection.
To date, breakthrough infections have been reported in a relatively low number of vaccinated individuals. However, scientists are wary about new variants that could evade immune protection and rapidly spread in a highly vaccinated community. Following the winter outbreak of the Epsilon variant in 2020-2021, a sharp decline in the number of COVID-19 cases was reported in San Francisco, California. After full-fledged mass vaccination programs commenced, researchers found that the number of COVID-19 cases continued to decline gradually between February 2021 and June 2021.
A reduced number of cases were observed, despite a nationwide outbreak of the Alpha variant and the continual introduction of other VoIs and VoCs in the United States during this period.
However, in the latter part of June 2021, a surge in the number of cases was observed in this nation, owing to the prevalence of the Delta variant. Less research is available that explores the link between the rise in vaccine breakthrough cases and infection by SARS-CoV-2 variants.
Vaccine breakthrough and SARS-CoV-2 variants
A new study published on the medRxiv* preprint server focused on studying breakthrough infections in a highly vaccinated community owing to the emergence of SARS-CoV-2 variants. In this study, researchers have conducted whole-genome sequencing and estimated the viral loads from nasal swab samples collected from vaccinated participants who contracted COVID-19.
In this study, researchers performed SARS-CoV-2 whole-genome sequences and measured viral loads from 1,373 COVID-19 infected individuals residing in the San Francisco Bay Area between February 1, 2021, and June 30, 2021. Researchers observed that 9.1% of the individuals included in the sample were vaccine breakthrough infection cases. The findings of the current study are in line with previous studies that reported a reduction in the number of hospitalizations and mortality in vaccinated individuals compared to unvaccinated people.
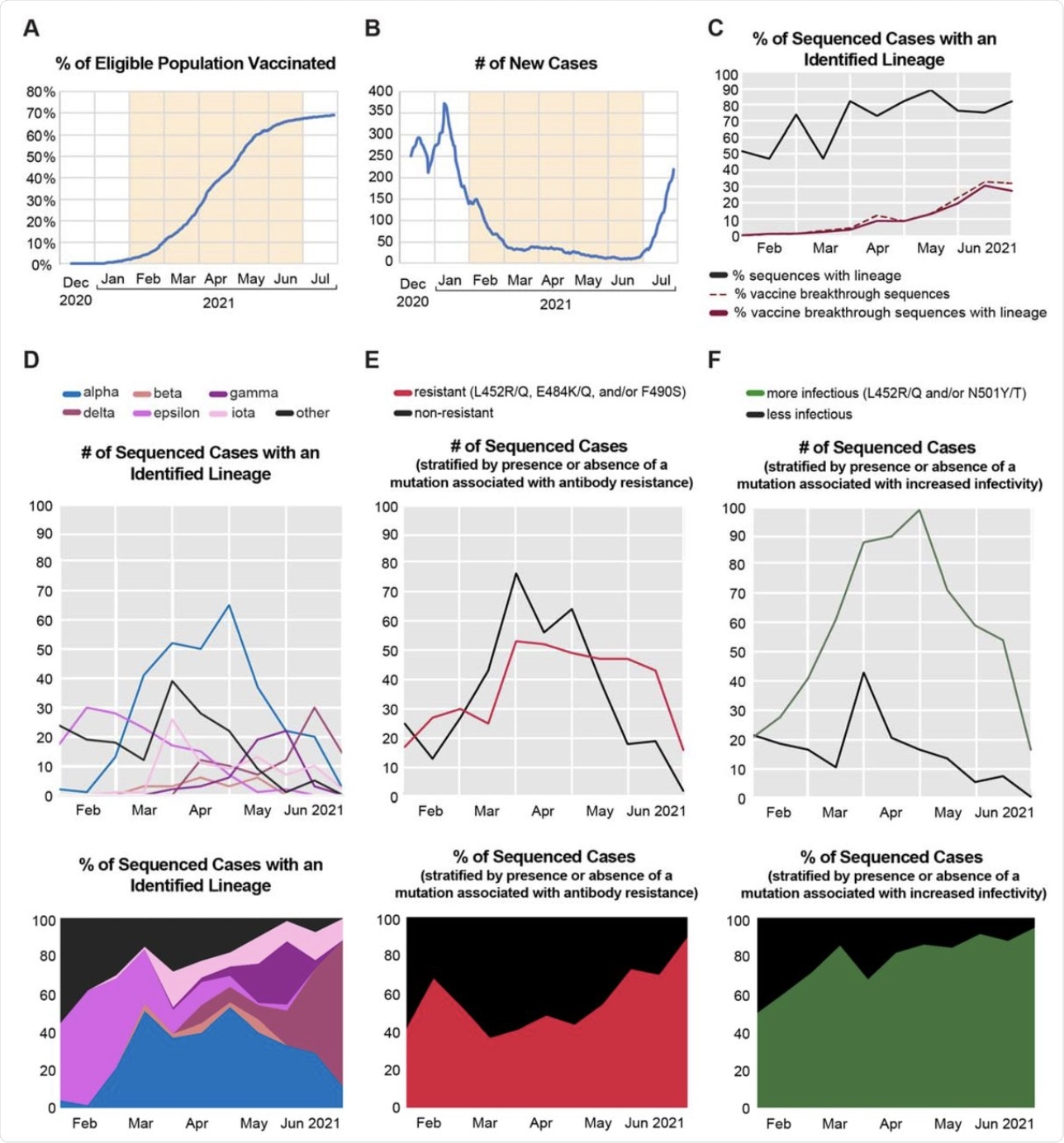 (A) Plot showing the percentage of eligible individuals in San Francisco County who had received an FDA-authorized vaccine from the beginning of mass vaccine rollout until June 30, 2021. The peach-colored shaded area denotes the study timeframe for sample collection. (B) Plot showing the 7-day rolling average number of new SARS-CoV-2 positive cases in San Francisco County. (C) Plot showing the proportions of total vaccine breakthrough sequences (denoted by the dotted line) and vaccine breakthrough sequences with identified lineages, relative to the total number of sequenced cases, and aggregated biweekly. (D-F) Plots showing the counts (top) and proportion (bottom) of SARS-CoV-2 positive sequenced cases aggregated biweekly and stratified by (D) lineages identified by Pangolin algorithm36, (E) presence/absence of mutations associated with antibody resistance, and (F)presence/absence of mutations associated with increased infectivity.
(A) Plot showing the percentage of eligible individuals in San Francisco County who had received an FDA-authorized vaccine from the beginning of mass vaccine rollout until June 30, 2021. The peach-colored shaded area denotes the study timeframe for sample collection. (B) Plot showing the 7-day rolling average number of new SARS-CoV-2 positive cases in San Francisco County. (C) Plot showing the proportions of total vaccine breakthrough sequences (denoted by the dotted line) and vaccine breakthrough sequences with identified lineages, relative to the total number of sequenced cases, and aggregated biweekly. (D-F) Plots showing the counts (top) and proportion (bottom) of SARS-CoV-2 positive sequenced cases aggregated biweekly and stratified by (D) lineages identified by Pangolin algorithm36, (E) presence/absence of mutations associated with antibody resistance, and (F)presence/absence of mutations associated with increased infectivity.
The authors of this study indicated that fully vaccinated individuals were at a higher risk of being infected by variants containing mutations such as L452R, L452Q, E484K, and/or F490S as compared to unvaccinated persons. These mutations are associated with decreased antibody neutralization.
This study revealed no significant difference in viral load between vaccinated and fully vaccinated individuals, regardless of lineage. Scientists have estimated viral loads using Ct values.
The viral loads were reported to be significantly greater in symptomatically infected individuals as compared to asymptomatic vaccine breakthrough cases. Additionally, the researchers revealed similar viral loads in symptomatic vaccine breakthrough infections and unvaccinated infections.
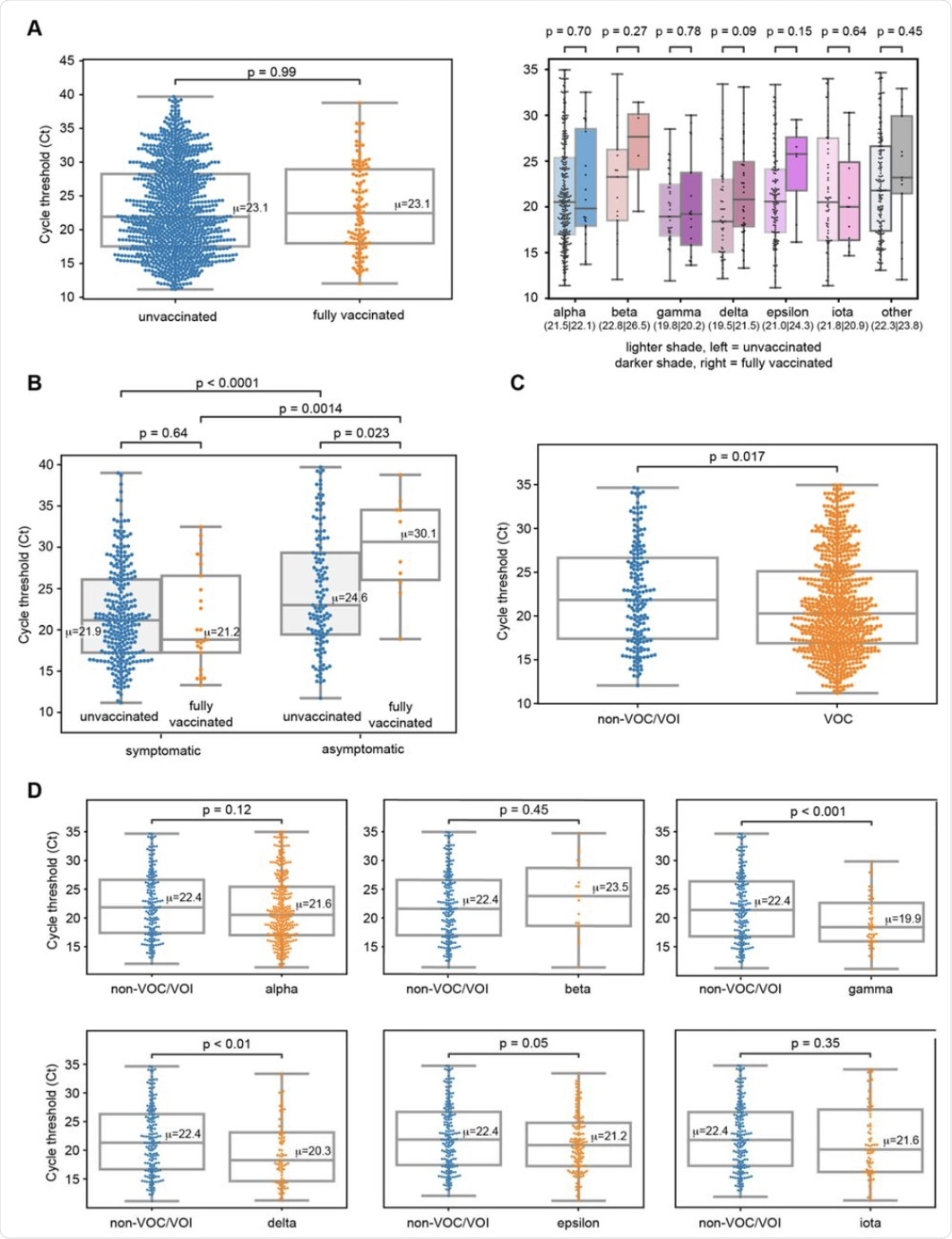 (A) Grouped box-and-whisker plots and swarm plots showing the differences in mean cycle threshold (Ct) values between vaccinated and unvaccinated cases overall (left) and stratified according to lineages (right). There were no significant differences in viral loads (inversely proportional to the Ct value) in both comparisons. Notably, higher viral loads were observed in gamma and delta unvaccinated cases, but the differences were not statistically significant (p > 0.05). (B) Box-and-whisker and swarm plots showing the differences in viral loads between symptomatic and asymptomatic cases. Each group was further subdivided into fully vaccinated and unvaccinated cases. Each pairwise comparison was statistically significant except for symptomatic unvaccinated and symptomatic vaccinated. (C) Box-and-whisker and swarm plots showing the differences in viral load between lineages identified as VOC/VOI (variant of concern/variant of interest) and other lineages that are not VOCs or VOIs (“non-VOC/VOI”). In this study, identified VOCs/VOIs included alpha, beta, gamma, delta, epsilon, and iota variants, following the World Health Organization (WHO) nomenclature scheme. (D) Box-and-whisker and swarm plots showing differences in viral loads between each VOC/VOI and non-VOC/VOI. Blue-colored dots denote non-VOC/VOI data points while orange-colored dots denote VOC/VOI data points. For all box-and-whisker plots, the box outlines denote the interquartile ratio (IQR), the solid line in the box denotes the mean (μ) Ct value, and the whiskers outside the box extend to the minimum and maximum fold enrichment points. For the lineage plots in 3A (right), the mean Ct values corresponding to unvaccinated and fully vaccinated cases are provided as μunvaccinated|μvaccinated in parentheses next to the name. Welch’s t-test was used for significance testing.
(A) Grouped box-and-whisker plots and swarm plots showing the differences in mean cycle threshold (Ct) values between vaccinated and unvaccinated cases overall (left) and stratified according to lineages (right). There were no significant differences in viral loads (inversely proportional to the Ct value) in both comparisons. Notably, higher viral loads were observed in gamma and delta unvaccinated cases, but the differences were not statistically significant (p > 0.05). (B) Box-and-whisker and swarm plots showing the differences in viral loads between symptomatic and asymptomatic cases. Each group was further subdivided into fully vaccinated and unvaccinated cases. Each pairwise comparison was statistically significant except for symptomatic unvaccinated and symptomatic vaccinated. (C) Box-and-whisker and swarm plots showing the differences in viral load between lineages identified as VOC/VOI (variant of concern/variant of interest) and other lineages that are not VOCs or VOIs (“non-VOC/VOI”). In this study, identified VOCs/VOIs included alpha, beta, gamma, delta, epsilon, and iota variants, following the World Health Organization (WHO) nomenclature scheme. (D) Box-and-whisker and swarm plots showing differences in viral loads between each VOC/VOI and non-VOC/VOI. Blue-colored dots denote non-VOC/VOI data points while orange-colored dots denote VOC/VOI data points. For all box-and-whisker plots, the box outlines denote the interquartile ratio (IQR), the solid line in the box denotes the mean (μ) Ct value, and the whiskers outside the box extend to the minimum and maximum fold enrichment points. For the lineage plots in 3A (right), the mean Ct values corresponding to unvaccinated and fully vaccinated cases are provided as μunvaccinated|μvaccinated in parentheses next to the name. Welch’s t-test was used for significance testing.
A longitudinal antibody analysis showed vaccine breakthrough cases are commonly linked to low or undetectable qualitative and neutralizing antibody levels in response to vaccination. In this study, the researchers identified three breakthrough infection cases from the Alpha variant. All patients were found to be immunocompromised and, as a result, failed to generate vaccine-induced antibodies.
In this study cohort, one Delta breakthrough infection was reported in a patient who had received the Johnson and Johnson COVID-19 vaccine.
Limitations
One of the limitations of this study is that some of the clinical data collected from retrospective medical chart reviews were incomplete. Additionally, among the study cohort, the number of vaccinated persons with breakthrough infections was relatively small of 125, among which only 39 cases were accompanied by proper clinical and epidemiologic metadata.
Due to the lack of contact tracing metadata, the researchers were not able to evaluate transmission and secondary attack rates from vaccinated persons to exposed contacts.
*Important notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- Servellita, V., Morris, M., Sotomayor-Gonzalez, A., et al. (2021) Predominance of antibody-resistant SARS-CoV-2 variants in vaccine breakthrough cases from the San Francisco Bay Area, California. medRxiv. doi:10.1101/2021.08.19.21262139. https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v1.
Posted in: Medical Research News | Disease/Infection News | Healthcare News
Tags: Antibodies, Antibody, Coronavirus, Coronavirus Disease COVID-19, CT, Efficacy, Genome, Healthcare, Mortality, Pandemic, Research, Respiratory, SARS, SARS-CoV-2, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, Syndrome, Vaccine, Virus

Written by
Dr. Priyom Bose
Priyom holds a Ph.D. in Plant Biology and Biotechnology from the University of Madras, India. She is an active researcher and an experienced science writer. Priyom has also co-authored several original research articles that have been published in reputed peer-reviewed journals. She is also an avid reader and an amateur photographer.
Source: Read Full Article